Injecting insulin correctly
For T1s, insulin is not medicine, it’s oxygen. We need it daily to stay alive. Unlike other medications, this can only be administered into the subcutaneous layer of the skin. If it's taken orally, the digestive juices in the stomach and intestine will break down the insulin before it has a chance to get into the bloodstream to do its job!
During my initial interactions with the diabetes educator at my endocrinologist’s office after my diagnosis, I learnt how to take an insulin shot on my stomach (bolus) and thigh (basal). The educator told me about site rotation but did not touch upon the common side effect of injecting at the same place, called lipohypertrophy.
Lipohypertrophy is a lump under the skin caused by accumulation of extra fat at the injection site which may be unsightly, mildly painful, and may change the timing or completeness of insulin action.
However sometimes it’s not even visible. It's possible to have it under the skin as well.
Irrespective of the diabetes equipment that you use (pump or MDI), lipohypertrophy can happen to anyone if you do not rotate your injection sites periodically.
Site Rotation
The thought behind site rotation is to avoid injecting in the same spot within a short duration of time. It’s advised to rotate injection sites to avoid this painful condition. For mealtime insulin, site rotation should be done in the same area to ensure consistency in the absorption of insulin.
If we use the affected site to take insulin, the insulin won't absorb properly and the site won't heal. Small children sometimes want to inject at the same spot because it hurts less but it's not the correct thing to do.
Do not inject the affected area for extended periods to aid the healing process.
Methods to administer insulin
With advent of technology, insulin can be administered using an insulin pen that uses needles or it can be taken using a syringe or even a pump. Traditionally, needles used in insulin therapy were 12.7 mm in length. Recent research shows that smaller 8 mm, 6 mm, and 4 mm needles are just as effective, regardless of body mass.
Choose the thinnest needle possible. Remember, the higher the gauge, the thinner the needle.
In my conversation with fellow T1s who have been taking insulin for over two decades, they said that taking insulin shots today is lesser painful than it was 20 years ago.
Injection sites
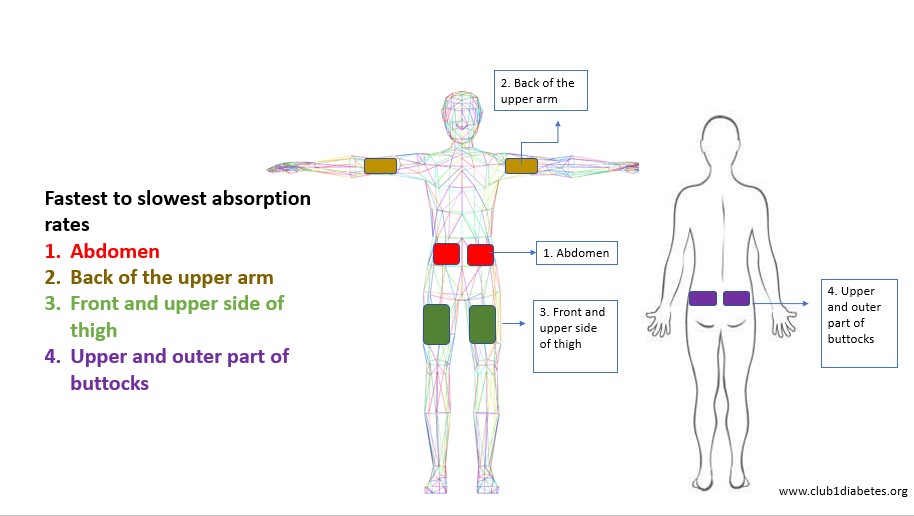
Enough literature on the internet explains the different sites that can be used to administer insulin. The absorption rate for insulin differs for every different site. Depending upon the type of insulin (basal or bolus) being injected, the site should be decided.
1. Stomach
Abdomen (and even the lower back and love handles) is recommended for injecting bolus insulin as it has the fastest absorption rate. The abdomen has a good amount of fat to aid the insulin administration. Another reason for preferring the abdomen is that it’s easily accessible. For meal time insulin, if the injection is being taken in the abdomen then please note :
- Select a site below your ribs and above your pubic region. Leave around 2 inches from your navel.
- Leave 1 finger gap between every successive shot to ensure you don’t take insulin at the same spot. Refer the image to understand how to pick successive injection spots.
- Make sure that each injection is about an inch (two finger-widths) from the last injection.
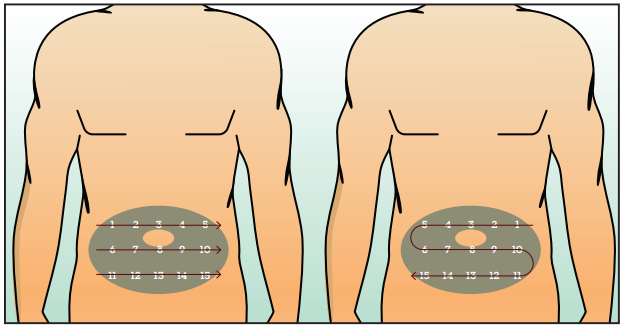
Like in the image, you must rotate sites to avoid developing lipohypertrophy. There should be a gap of about 1-2 cm between each consecutive shot.
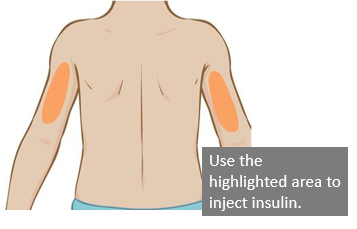
2. Arms
Arms have an absorption rate that is slower than the abdomen, however it can still be used to take bolus insulin. Use the fatty area on the back of your arm, between your shoulder and elbow. Please avoid the muscle in the shoulder while injecting as intra-muscular injections work extremely fast and could lead to hypos quickly.
3. Thighs
I use my thighs to take basal as the absorption rate is slowest. It's not advised to take bolus on the thighs. You can inject into the top and outer areas of your thigh, about 4 inches down from the top of your leg and 4 inches up from your knee.

4. Buttocks
You can use the buttocks to inject bolus and basal insulin both. The absorption rate is slower than the abdomen though.
Things to remember
1. Be consistent with the area you use to administer insulin as the absorption rate differs for each site.
2. In case you are on MDI, please ensure that the pen is used by a single person. Even after changing needles, its not advised that two people use the same pen.
3. Please ensure you dispose your needles and cartridges correctly.
4. Always disinfect the site and avoid taking a shot through clothes.
5. Inject insulin at room temperature. Cold insulin has a tendency to sting.
6. Change your needles and infusion sets regularly.
7. Do not rub the area after injecting.
8. To ensure that the insulin does not leak, “pinch” the area and count to 10 after taking a shot (especially for pens).
9. Check for lipohypertrophy at least 1-2 times a year by your doctor and self check more often.
SUPPORT BLUE CIRCLE DIABETES FOUNDATION
We need your help and support to continue to grow, expand and touch the lives of countless people in the diabetes community. Every little bit helps us in sustaining this endeavour. Our NGO is registered under Section 80G of the Income Tax Act, India.
Click here to donate
